Aside from insulin resistance, discussed in “The Real Pandemic Is Insulin Resistance,” mounting research reveals vitamin D deficiency is one of the primary risk factors for severe COVID-19 infection, hospitalization, complications and death.
Vitamin D can strengthen your immune system in a matter of a few weeks, and according to recent research, correcting vitamin D deficiency could save thousands of lives in Great Britain alone. As reported by conservative member of the British Parliament David Davis and writer Matt Ridley in a September 26, 2020, article in The Telegraph:1
“As we face six tough months of curfews, isolation and economic misery, with vaccines a distant hope, testing struggling to control the virus, and the hospitalization rate once again rising, it’s surely time to try anything reasonable to slow the pandemic down.
There is one chemical that is known to be safe, known to be needed by many people anyway, known to have a clinically proven track record of helping people fight off respiratory diseases, and is so cheap no big firm is pushing it: vitamin D. It is not a silver bullet, but growing evidence suggests that it might help prevent COVID turning serious in some people.”
Randomized Control Trial Confirms Vitamin D Cuts ICU Rates
As reported by The Telegraph, while initial support for vitamin D relied on data showing correlations between vitamin D levels and infection rates and COVID-19 outcomes, we now have a randomized, controlled trial backing it up.
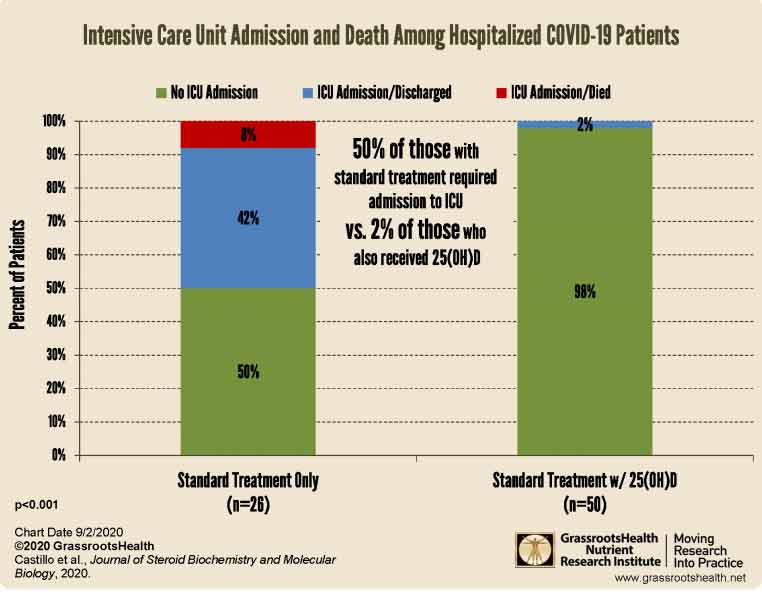
The study,2,3,4,5 published online August 29, 2020, found hospitalized COVID-19 patients who received supplemental calcifediol (a vitamin D3 analog also known as 25-hydroxycholecalciferol or 25-hydroxyvitamin D) in addition to standard of care — which included the use of hydroxychloroquine and azithromycin — had significantly lower intensive care unit admissions. It also eliminated deaths.
Patients in the vitamin D arm (50 out of 76 enrolled patients) received 532 micrograms of calcifediol on the day of admission (equivalent to 106,400 IUs of vitamin D6) followed by 266 mcg on Days 3 and 7 (equivalent to 53,200 IUs7). After that, they received 266 mcg once a week until discharge, ICU admission or death.
Of those receiving calcifediol, only 2% required ICU admission, compared to 50% of those who did not get calcifediol. In other words, the addition of vitamin D reduced a patient’s risk of needing intensive care 25-fold.8
What’s more, none of those in the vitamin D arm died, compared to 7.6% in the standard care group. The graph below, created by GrassrootsHealth,9 illustrates the difference in ICU admissions and deaths between the two trial groups.
As noted by Davis and Ridley:10
“While the sample is too small to conclude that vitamin D abolishes the risk of death in COVID patients, it is nonetheless an astonishing result, and corresponds with Prof Backman’s assertion that correcting vitamin deficiency might cut mortality by half. The Government should now act on this latest evidence.
Vitamin D supplementation is cheap — it costs less than a penny a pill — and readily available. If you allocated this to the identified comorbidity risk group it would cost £45 million: to these, plus to every ethnic minority citizen, about £200 million, to every obese person somewhat more. These costs are trivial rounding errors by comparison with the costs of lockdown.
With hospitals already facing pressures from influenza during the winter months, any way of reducing this strain should be taken up. This will no doubt save thousands of lives in any second wave. There is now no reason not to act.”
Vitamin D Sufficiency Cuts Fatalities in Half
Another study,11,12,13 published online September 25, 2020, in PLOS ONE, found COVID-19 patients with a vitamin D level of at least 30 ng/mL had a significantly lower risk of adverse clinical outcomes, including a 51.5% lower risk of dying.
Hospital data of 235 COVID-19-positive patients were analyzed for this study. Of those, 74% had severe symptoms and 32.8% were vitamin D deficient. As reported by the authors:14
“After adjusting for confounding factors, there was a significant association between vitamin D sufficiency and reduction in clinical severity, inpatient mortality serum levels of C-reactive protein (CRP) and an increase in lymphocyte percentage.
Only 9.7% of patients older than 40 years who were vitamin D sufficient succumbed to the infection compared to 20% who had a circulating level of 25(OH)D< 30 ng/ml.
The significant reduction in serum CRP, an inflammatory marker, along with increased lymphocytes percentage suggest that vitamin D sufficiency also may help modulate the immune response possibly by reducing risk for cytokine storm in response to this viral infection.
Therefore, it is recommended that improving vitamin D status in the general population and in particular hospitalized patients has a potential benefit in reducing the severity of morbidities and mortality associated with acquiring COVID-19.”
One of the co-authors of this study was Dr. Michael Holick, a professor of medicine, physiology and biophysics and molecular medicine at Boston University School of Medicine. Holick is also on GrassrootsHealth’s vitamin D expert panel,15 and is widely recognized as one of the leading vitamin D experts in the world.
Higher Vitamin D Lowers Risk of Positive SARS-CoV-2 Test
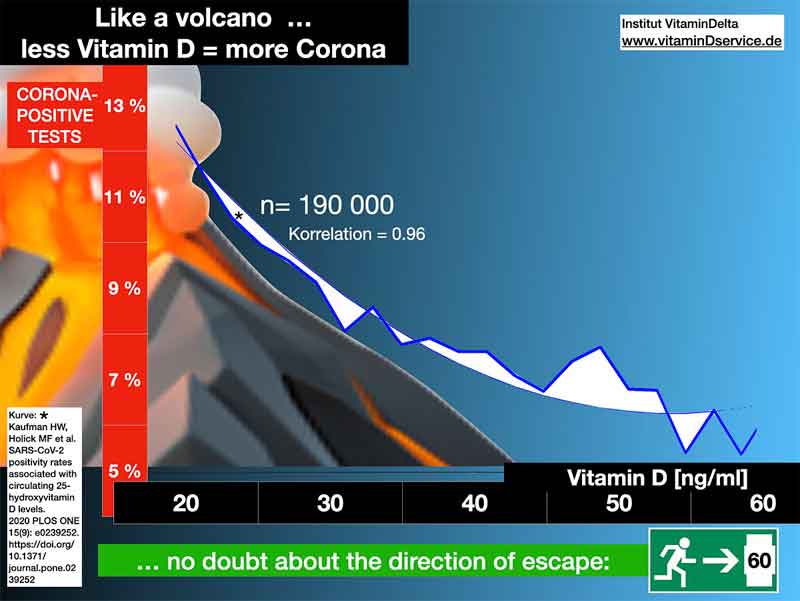
In a September 17, 2020, paper,16 Holick and his team also reported findings showing that people with lower vitamin D levels in their blood had a significantly higher risk of testing positive for SARS-CoV-2.
Analysis of vitamin D results from the preceding 12 months and SARS-CoV-2 test data from mid-March through mid-June 2020 from 191,779 patients revealed the higher the vitamin D level the lower the risk of testing positive for SARS-CoV-2.
People with a vitamin D level of at least 55 ng/mL (138 nmol/L) had a 47% lower SARS-CoV-2 positivity rate compared to those with a level below 20 ng/mL (50 nmol/L).17
Even after adjustment for gender, age, ethnicity and latitude, the risk of having a positive test result was 43% lower among those with a vitamin D level of 55 ng/mL compared to those with a level of 20 ng/mL.
Granted, there are many reasons to be suspicious of COVID-19 tests. They may well be worthless, considering the high rate of false positives. Still, at present, it’s the only metric we have to assess the potential value of any given intervention.
Experts Weigh in on Vitamin D
In the video above, Holick, along with Rufus Greenbaum, a citizen scientist in the U.K., physicist Gareth Davies, Ph.D., and Drs. William Grant and David Grimes present important new information about vitamin D as it relates to COVID-19:
• Holick discusses his two studies summarized above. He also reviews:
◦ The importance of vitamin D for healthy immune function and how it affects cytokine production and cytokine storms
◦ Minimum and ideal vitamin D levels
◦ Suggested minimum dosages and evidence showing vitamin D is nontoxic even at doses of 20,000 IUs a day
◦ How to calculate your vitamin D production from sun exposure using the D-Minder app,18 which he helped develop
• Grant provides an overview of more than 15 vitamin D trials published around the world, showing:
◦ Vitamin D lowers your risk of testing positive for SARS-CoV-2 and/or being diagnosed with COVID-19
◦ Reduces your risk of severe infection
◦ Improves clinical outcomes in hospitalized COVID-19 patients and reduces need for intensive care and/or mechanical ventilation
◦ Increases survival in COVID-19 patients with acute respiratory failure
◦ Lowers COVID-19 related fatality rates, and more
• Davies explains how his team used artificial intelligence and causal interference to demonstrate the influence of vitamin D deficiency on COVID-19 outbreaks and illness severity around the world.
According to Davies, the data unequivocally proves vitamin D deficiency worsens COVID-19 outcomes, and the biological mechanisms behind these effects — including vitamin D’s effect on your innate immune system, adaptive immune system, ACE2 receptors and renin-angiotensin system — are well-documented
• Grimes reviews and explains how various studies showing a correlation between vitamin D levels and COVID-19 risks end up fulfilling Bradford Hill’s criteria for causation.
As explained by Grimes, “proof” is “the fulfilment of predetermined criteria.” Proof is never absolute. Bradford Hill criteria are used in medical science when trying to establish an argument for causation. These criteria, which are explained in further detail by Grimes, include the following.19
|
Strength of association |
Consistency |
Specificity |
|
Temporality/temporal sequence |
Plausibility |
Biologic rationale |
|
Coherence |
Experimental evidence |
Analogous evidence |
If these criteria are satisfactorily fulfilled, you have pragmatic proof of causation — in this case that vitamin D deficiency has a direct impact on COVID-19. According to Grimes:
“The evidence for vitamin D is overwhelming, so my conclusion is that during a pandemic, all people should take a vitamin D supplement.”
• Lastly, Greenbaum reviews U.K. data showing the level of vitamin D deficiency at various times of year, and lays out a plan of action moving forward
Britons Are Sorely Deficient in Vitamin D
As noted by Greenbaum, the information presented is aimed at everyone, including national and local health policy experts, politicians, health care professionals, insurance companies and laypersons.
Additional information can be found on vitaminduk.com. There, you can also download each expert’s presentation. For clarity, the U.S. and Europe use different units of measure for vitamin D. The U.S. uses ng/mL and Europe, including the U.K. use nmol/L. You can easily translate ng/mL into nmol/L by multiplying the ng/mL measurement by 2.5.
For reference, GrassrootsHealth experts (which include Holick) recommend a vitamin D level between 40 ng/mL and 60 ng/mL (100 nmol/L to 150 nmol/L) for optimal health and disease prevention.
For bone health, a level of 30 ng/mL (75 nmol/L) is recommended. In the U.S., a vitamin D level below 20 ng/mL (50 nmol/L) is considered deficient, whereas the U.K. department of health defines deficiency as a level below 10 ng/mL (25 ng/mL).
According to Greenbaum’s data, many Britons are so deficient in vitamin D that to achieve a target level of 100 nmol/L or higher, they need to increase their blood levels of vitamin D by four to six times.
Now’s the Time to Optimize Your Vitamin D Level
As we move into fall in the Western Hemisphere, now’s the time to start optimizing your vitamin D level. Experts are already warning that SARS-CoV-2 may reemerge in the fall when temperatures and humidity levels drop, thereby increasing the virus’ transmissibility. Optimizing your vitamin D is particularly important if you are elderly or have darker skin. To make sure your immune system has a chance to work optimally, follow these three steps.
1. Measure your vitamin D — First, find out what your baseline vitamin D level is. This is done with a simple blood test. An easy and cost-effective way of doing this is to order GrassrootsHealth’s vitamin D testing kit.
Once you know what your blood level is, you can assess the dose needed to maintain or improve your level. Again, the ideal level you’re looking for is above 40 ng/mL, and ideally between 60 ng/mL and 80 ng/mL (European measurement: 100 nmol/L or, ideally, 150 nmol/L to 200 nmol/L).
2. Assess your individualized vitamin D3 dosage — The following chart can provide you with a basic starting point:

You can fine-tune your dosage further by taking into account your baseline vitamin D level. To do that, you can either use the chart below, or use GrassrootsHealth’s Vitamin D*calculator. (To convert ng/mL into nmol/L, simply multiply the ng/mL measurement by 2.5.)
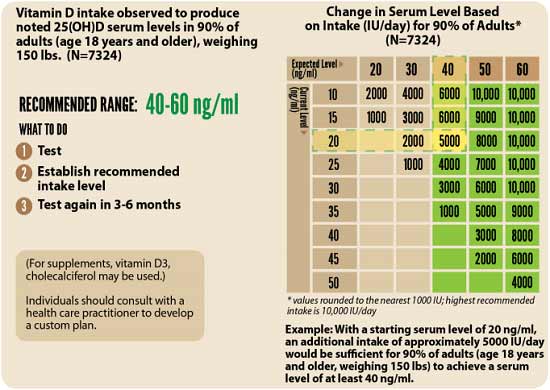
3. Retest — Lastly, you’ll need to remeasure your vitamin D level in three to six months, to evaluate how your sun exposure and/or supplement dose is working for you.
For more details about how vitamin D can help prevent and combat COVID-19, see my special report, available for free download on StopCOVIDcold.com (no opt-in required). There, you can also find a two-minute COVID risk quiz to assess your personal risk for developing COVID-19.
from Articles https://ift.tt/2Sotb1s
via IFTTT






0 comments:
Post a Comment