Go to Blogger edit html and find these sentences.Now replace these sentences with your own descriptions.This theme is Bloggerized by Lasantha Bandara - Premiumbloggertemplates.com.
Go to Blogger edit html and find these sentences.Now replace these sentences with your own descriptions.This theme is Bloggerized by Lasantha Bandara - Premiumbloggertemplates.com.
Go to Blogger edit html and find these sentences.Now replace these sentences with your own descriptions.This theme is Bloggerized by Lasantha Bandara - Premiumbloggertemplates.com.
Go to Blogger edit html and find these sentences.Now replace these sentences with your own descriptions.This theme is Bloggerized by Lasantha Bandara - Premiumbloggertemplates.com.
Go to Blogger edit html and find these sentences.Now replace these sentences with your own descriptions.This theme is Bloggerized by Lasantha Bandara - Premiumbloggertemplates.com.
Workers at 30 HCA Healthcare hospitals in multiple states picketed on Friday, advocating for progress in contract negotiations and higher quality patient care.
The day of action, conducted by SEIU Healthcare members, marked the expiration of a union contract covering 3,000 HCA workers in California. Contracts for another 19,000 workers at HCA-owned hospitals in Florida, Nevada, Texas and Kansas are set to expire by September.
At HCA’s Riverside Community Hospital in southern California, thousands of clinicians gathered, demanding the system address issues of low staffing and patient safety and claiming HCA has not made significant headway in negotiating a new agreement that benefits staff and patients.
“Today’s day of action is all about safe staffing and patient care,” said Raymond Valdivia, a lab assistant and phlebotomist at the hospital in Riverside, California and a SEIU union leader. “We’re out here so HCA and Riverside Community Hospital listen to our requests when it comes to staffing ratios, better supplies and equipment that we need so we can take care of patients.”
Increasing staffing levels to meet hospital needs is also the main focus of contract negotiations, he said.
Even with the national nursing shortage, the health system always strives to reach agreements that are in the best interest of caregivers and patients, and has compensation and staffing levels in line with regulations and practices at other community hospitals, HCA said in an email statement.
“The SEIU has a history of attacking and bullying community hospitals with misleading information and staged events,” HCA said. “We expect a variety of deceptive labor union tactics like this as we continue our regular cycle of bargaining with the labor union.”
The push for improvement from union members comes amid allegations of patient safety issues and potential Medicare fraud at the health system.
The Health and Human Services Department is reviewing a letter from U.S. Rep. Bill Pascrell (D-N.J.) and the SEIU that claimed HCA forces its doctors to meet unofficial quotas for the number of patients admitted to the hospital.
In March, Sen. Marco Rubio (R-Fla.) and Rep. Gus Bilirakis (R-Fla.) wrote a letter to the CEO of HCA Florida Bayonet Point Hospital in Hudson, Florida, asking the facility’s leadership to address reports of unsanitary and unsafe practices.
The University System of Georgia Board of Regents voted Friday to approve Wellstar Health System’s proposed takeover of Augusta University Health System.
Wellstar, a nine-hospital system based in Marietta, Georgia, would become the corporate parent of Augusta Health System, which includes the 600-bed AU Medical Center, the Children’s Hospital of Georgia, the Georgia Cancer Center, the Roosevelt Warm Springs Rehabilitation and Specialty Hospitals and a physician practice. The transaction, which follows other recent health system affiliations with academic medical centers as they aim to bolster clinician recruitment and retention, is expected to close in the summer, pending regulatory approvals. The companies signed a letter of intent in December.
The deal comes on the heels of Wellstar closing Atlanta Medical Center, a 460-bed safety-net hospital and one of two Level 1 trauma centers in the city. Wellstar shut down the hospital in November, displacing low-income patients and provoking outcry from the community and from local and state officials.
Wellstar maintained that it wasn’t financially sustainable to keep Atlanta Medical Center open. Other area hospitals, such as Grady Memorial Hospital, have since experienced higher volumes and longer wait times. A Wellstar spokesperson did not say whether the deal with Augusta would have any impact on Atlanta Medical Center.
Under the agreement with Augusta, Wellstar pledged to invest nearly $800 million over 10 years in Augusta facilities and infrastructure, including building a new hospital in nearby Columbia County. The affiliation would increase the number of physicians trained in Georgia and advance research, Wellstar Health System President and CEO Candice Saunders said during a news conference Friday.
“We will train more physicians to help address the significant shortage of physicians in our state,” Saunders said.
The Wellstar board would become the fiduciary governing body for Augusta, which otherwise would continue to operate as it does today, the Wellstar spokesperson said. The Medical College of Georgia would remain independent from the combined entity, the spokesperson said.
Wellstar reported $105.8 million in operating income on $4.57 billion of revenue in fiscal 2022, which ended June 30. That was down from $377.1 million in operating income on $4.25 billion of revenue in fiscal 2021. The company’s days cash on hand dropped from 208 to 160 over that span.
Augusta, which generates roughly $1.1 billion in annual revenue, recorded operating losses for each of its last three fiscal years.
3 million Pennsylvanians need to renew Medicaid eligibility to continue state-sponsored health insur
3 million Pennsylvanians need to renew Medicaid eligibility to continue state-sponsored health insur
02:34
For millions of Americans who get medical care under Medicaid, the end of March marks a grim deadline. Starting April 1, states will start removing people from the government health insurance program for the poor, paring rolls that swelled during the pandemic.
The government estimates that 15 million people — or roughly 1 in 6 of the 84 million on Medicaid — will be kicked off the program. Here’s why this is happening and what people should know.
What’s happening to Medicaid?
During the pandemic, the government suspended procedures that would remove people from Medicaid. Before the crisis, people would regularly lose their Medicaid coverage if they started making too much money to qualify for the program, or if they moved out of state or gained health care coverage through their employer. That stopped once COVID-19 hit, causing Medicaid enrollment to grow by 5 million between 2020 and 2022.
Michigan Medicaid recipients must update information for redetermination
01:35
The Consolidated Appropriations Act, signed last December as the pandemic continued to ebb, instructed states to restart eligibility checks of every person currently on Medicaid. To stay on the rolls, individuals will have to fill out forms to verify their personal information, including their address, income and household size.
Who is affected?
People in danger of losing Medicaid coverage may have relocated or received an income boost that makes them ineligible.
“Millions of people, working adults, parents with children, will lose Medicaid when they try to re-enroll,” said Ellen Taverna, associate director of the Together for Medicaid program at Community Catalyst. Of those, she estimated 380,000 are working adults who won’t be eligible for other health coverage because they make too little to qualify for Obamacare subsidies, while making too much to sign up for Medicaid.
However, many are likely to drop out of the program for administrative reasons, such as not receiving a form they need to fill out to re-verify their income and eligibility.
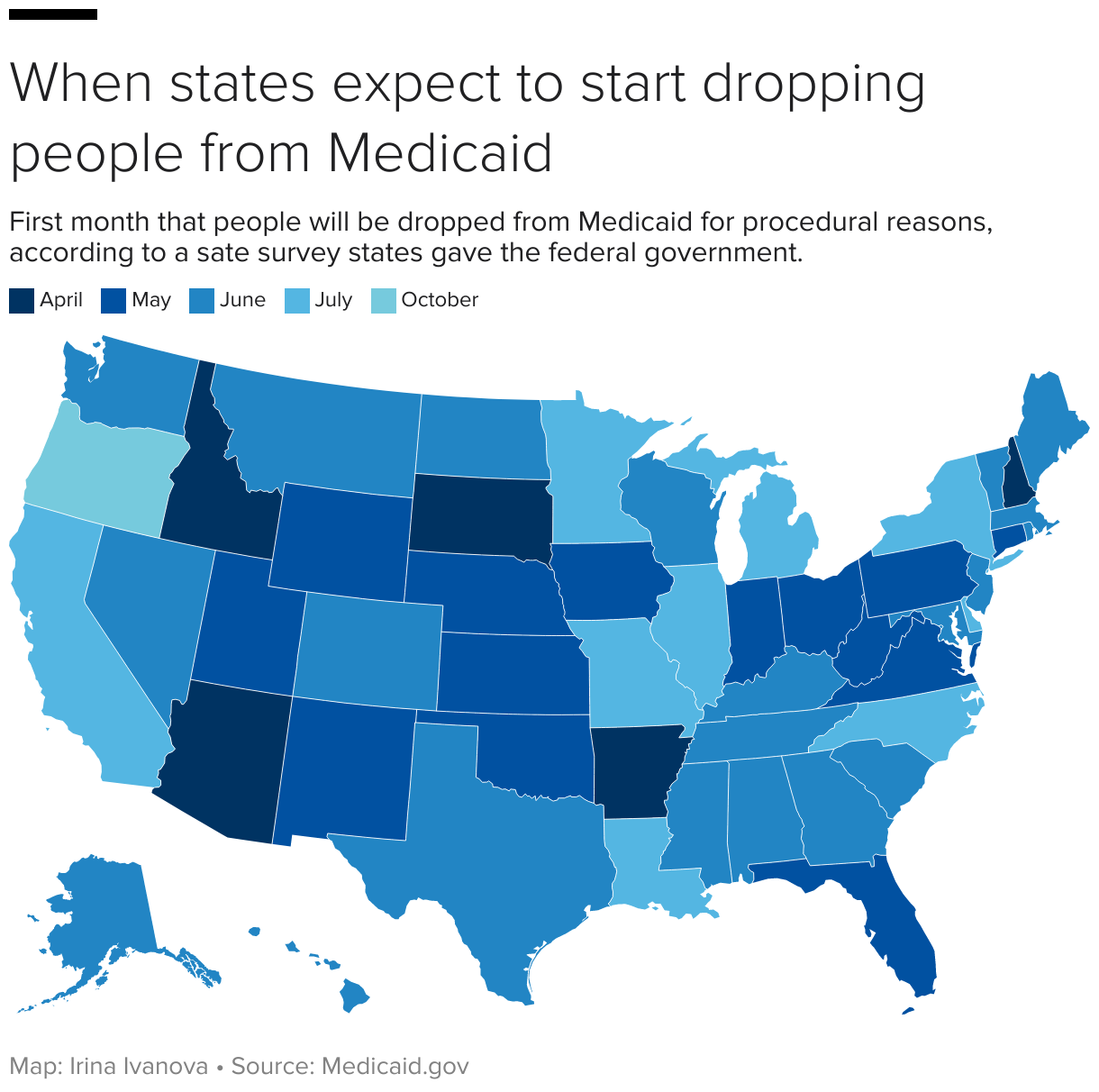
When are people losing coverage?
That depends on where you live in.
Some states have already started the disenrollment process. The Associated Press reported that no-longer-eligible Medicaid members could be removed as soon as April in these nine states: Arizona, Arkansas, Florida, Idaho, Iowa, New Hampshire, Ohio, Oklahoma and West Virginia.
But not all ineligible people will be dropped from the program at once, as states have set different timelines for re-checking eligibility of Medicaid patients. Most states are expected to take between nine months and a full year to complete the verification process.
How are states notifying people being about losing Medicaid?
As recently as December, two-thirds of adults in Medicaid households weren’t aware that the program rules were changing, according to a survey from the Robert Wood Johnson Foundation.
“Unfortunately we’re going to see it in real time, with children and people losing coverage simply because people are unaware of what’s happening,” Taverna said.
“That’s the concern, that people will go without coverage for months and then go through bureaucracy and red tape to have to reenroll.”
Bill of the Month: Woman mistakenly charged for shoulder surgery she never had
05:48
Health care advocates are urging people on Medicaid to update their contact information, including their home address, phone number and email, with the state.
If you rely on Medicaid, states will mail a renewal form to your home. The federal government also requires states to contact you in another way -– by phone, text message or email –- to remind you to fill out the form.
“A text might just grab someone’s attention in a way that would be more accessible,” said Kate McEvoy, executive director of the nonprofit National Association of Medicaid Directors.
While most states have already used texting for reminders to get a COVID-19 vaccine or attend an upcoming doctor’s visit, sending mass texts on Medicaid eligibility will be new, McEvoy said.
You will have at least 30 days to fill out the form. If you do not fill out the form, states will be able to remove you from Medicaid.
What options do people have if they lose Medicaid?
Some of those who won’t qualify for Medicaid coverage will be able to get health insurance from the Affordable Care Act’s marketplace for coverage, where private coverage subsidized by federal tax credits can cost as little as $10 a month, depending on a person’s income.
A special enrollment period for people dropped from Medicaid starts March 31 and will last through July 31, 2024, the Centers for Medicare and Medicaid Services said in January. People who lose Medicaid coverage can submit an application at any time during that period after losing coverage and will have up to 60 days to select their plans, CMS said.
It noted that consumers don’t need to wait until their Medicaid ends to apply for new coverage, but can start applying 60 days before their Medicaid is scheduled to end.
Still, coverage through the Obamacare marketplace or through an employer is often vastly different from what Medicaid offers.
“Even on employer-sponsored plans, copays and out-of-pocket costs may be higher than Medicaid, and that makes it unaffordable,” Taverna said.
People changing coverage will also need to check that their new insurance plans will still cover their doctors.
Business analyst Jill Schlesinger discusses health insurance options during open enrollment
05:00
What happens to kids enrolled in Medicaid?
More than half of U.S. children receive health care coverage through Medicaid or the Children’s Health Insurance Program. But even if an adult loses Medicaid coverage, it doesn’t mean their kids will.
Even if you receive a notice that you’re no longer eligible for Medicaid, it’s likely that your child still qualifies for the program or for health care coverage through CHIP. CHIP covers children whose families make too much money to qualify for Medicaid but don’t earn enough to afford private health insurance.
Between 80% and 90% of children will still be eligible for those programs, according to estimates from the Georgetown University Health Policy Institute’s Center for Children and Families.
“When a parent receives a message that they aren’t eligible anymore, they often assume their child is no longer eligible either,” Joan Alker, the center’s executive director, told the Associated Press. “It’s more common to find that the parent is no longer eligible for Medicaid, but the child still is.”
There could be more than just fashion risks involved when buying a pair of leggings or a raincoat.
Just how much risk is still not clear, but toxic chemicals have been found in hundreds of consumer products and clothing bought off the racks nationwide.
Thousands of perfluoroalkyl and polyfluoroalkyl substances, or PFAS, exist since the first ones were invented in the 1940s to prevent stains and sticking. PFAS chemicals are used in nonstick cookware, water-repellent clothing and firefighting foam. Their manufacture and persistence in products have contaminated drinking water nationwide. Also known as “forever chemicals,” these substances do not break down in the environment and can accumulate in our bodies over time.
Until now, federal regulations on PFAS in consumer products have largely focused on a handful of the older-generation forever chemicals, such as PFOA, or perfluorooctanoic acid. But new state-level laws are targeting all forever chemicals.
Consumers concerned about clothing are also turning to the courts. A torrent of recent class-action lawsuits claim brands falsely advertise their products as environmentally sustainable or healthy while containing toxic levels of PFAS chemicals. In January, Thinx, which makes reusable period underwear, agreed to pay up to $5 million to settle a suit. Another lawsuit, against REI, largely targeting its raincoat line, is proceeding in court.
From production to being worn, washed, and then disposed, “PFAS in clothing and textiles can lead to harmful exposures,” claimed Avinash Kar, a senior attorney at the National Resources Defense Council, an international nonprofit environmental advocacy organization.
Although the full health risks of wearing togs alleged to be toxic are still unknown, the potential implications are wide-reaching. A report from the National Academies of Sciences, Engineering, and Medicine linked PFAS exposure to cancer, thyroid dysfunction, small changes in birth weight, and high cholesterol, among other concerns.
So how concerned should consumers be about wearing clothing with forever chemicals in them?
PFAS have been found in a wide variety of garments such as rain jackets, hiking pants, shirts and yoga pants and sports bras made by popular brands like Lululemon and Athleta.
Forever chemicals are used as surface treatments to block water and stains. In fact, a 2022 report by Toxic-Free Future, an environmental health research and advocacy organization, found that nearly three-quarters of products labeled as water- or stain-resistant tested positive for them.
The group points to research demonstrating that fabrics with that type of PFAS, called side-chain fluorinated polymers, emit volatile chemicals into the air and, when washed, into the water. “What you can expect is that a raincoat that has this surface treatment, over time, is releasing PFAS to the environment,” said Erika Schreder, Toxic-Free Future’s science director.
PFAS can also be used as a membrane — a thin layer sandwiched in the fabric that blocks water from passing through. This technology is found in products made with Gore-Tex. Such breathable yet waterproof layers of fabric are used in jackets, pants, boots, and gloves in dozens of brands of outdoors wear. Sometimes, garments have both membranes and surface treatments.
A study published last year by the American Chemical Society found textile products sold in the U.S. and Canada contained high concentrations of PFAS in materials used in children’s uniforms marketed as stain-resistant.
“This was concerning to us because these uniforms are on up to eight or 10 hours a day, every day, by children during their school year,” said Marta Venier, an assistant professor at Indiana University-Bloomington and co-author of the study. “Children are particularly susceptible to exposure to chemicals because their organs are still developing.”
But skin-touching fabric is only one way people are likely to be exposed to these chemicals. PFAS have found their way into most households through water, air, dust, and soap. PFAS can also shed from carpeting or furniture, as well as fabric treatments sprayed on furniture and clothing.
Studying skin or “dermal exposure” from wearing fabric is particularly tricky. Just because a product contains PFAS doesn’t mean the chemical will travel from that jacket or pair of shorts across the skin into the bloodstream, said Stuart Harrad, a professor of environmental chemistry at the University of Birmingham.
So far, Harrad has found that PFAS can end up — either from fabric or dust particles — in the skin’s oil and sweat. But more research needs to be done to examine whether those chemicals transfer into the blood. “From what we’ve seen, it’s certainly something that we shouldn’t be ignoring,” he said.
In general, however, it’s harder for PFAS chemicals to enter the body through transdermal exposure than through the digestive system, said Dr. Ned Calonge, associate dean for public health practice of the Colorado School of Public Health who co-authored the national academies’ report.
Levi Strauss has halted using the chemicals. Other brands, such as Patagonia, L.L. Bean, Lululemon and Eddie Bauer, have pledged to phase them out in the next few years. In late February, REI released updated standards that require most cookware and textile products to be PFAS-free by fall 2024. The retailer said in a statement last year that it has been “working for years to phase out PFAS” and is “testing new alternatives.”
W.L. Gore & Associates, inventor of Gore-Tex and a giant manufacturer of weather-repellent fabric, said it plans to “transition the vast majority of its consumer portfolio by end of 2025.” Last year, the company debuted a membrane that uses non-fluorinated materials and can be found in jackets sold by Arc’teryx, Patagonia, and other brands.
Still, without oversight, corporate commitments are not a guarantee, and there’s always concern of contamination, PFAS experts said. Gore, for example, said years ago that the company had eliminated PFOA from its materials. But in its testing last year, Toxic-Free Future found it in REI Gore-Tex rain jackets. Gore spokesperson Amy Calhoun rebutted those findings and said the company considers itself a leader in “responsible chemical management.”
People in the chemical field view this as an inflection point and are watching closely as companies phase out forever chemicals and pressing for transparency about what alternatives are chosen and how safe they might be.
The EPA has set out to regulate some older-generation chemicals generally found in imported products. Those have also been banned in the European Union and phased out by major U.S. manufacturers, often replaced by newer-generation PFAS, which leave the body more swiftly and are less likely to build up in organs. “When discussing the broad group of chemicals known as PFAS, it is important to note not all PFAS are the same,” said Calhoun. Some Gore products use PTFE, a polymer the company says is “of low concern.” According to a growing body of research, though, these newer PFAS often have similar levels of toxicity.
Stricter, state-level bans targeting apparel are rolling out. Maine now requires companies to report PFAS in their products to state officials. The chemicals will be fully banned there by the start of 2030, while Washington state will restrict PFAS in apparel as well as in other consumer products by 2025.
The most important legislation has come in two states with large consumer markets that manufacturers would be loath to avoid, effectively setting a standard for the nation. A New York law signed in late December bans the sale of garments with PFAS by the end of 2023. A California law passed last year restricts companies from manufacturing, distributing, or selling PFAS-containing clothing beginning in 2025, but those rules won’t apply to extreme weather and personal protective apparel until 2028.
So where does that leave consumers? Calonge said that people who already have high levels of PFAS in their blood serum should have a heightened sense of awareness about the clothing they wear. Community-level blood testing is underway in areas with known PFAS exposure, but individuals can also seek it out by asking their doctors.
“That’s when I would make a decision to not wear clothing that I know has PFAS in it,” he said.
Without sound evidence linking skin exposure from clothing to upticks in PFAS in blood serum levels, Calonge said, for now, decisions are largely left up to risk tolerance.
KHN(Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs atKFF(Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Sophia Antipolis, France & Brussels, Belgium, 30 March 2023 – Enreach for Service Providers, part of Enreach — the fast-growing European contact leader — has today announced a strategic partnership with Belgian-based Netaxis, a technology innovator delivering Fusion. This API integration layer converges multiple apps and systems into one simplified environment across various sources, including cloud unified communications (UC) platforms, BSS/OSS, and applications.
Service providers can take advantage of the fast-growing and profitable UC market through the combined solution of Enreach UP and Netaxis Fusion. The solution enables service providers to offer their customers a complete suite of UC features, such as contact centre solutions, meeting and collaboration tools, voice and video calling, messaging, UC connectivity and more. These features can help customers improve their productivity, communication, employee, and customer experience.
Enreach UP and Netaxis Fusion are both highly automated solutions that simplify the delivery and management of UC services. Service providers can use the combined solution to provision, configure, monitor, troubleshoot, and update UC services with ease and speed. This reduces operational costs and increases customer satisfaction. The solution also allows service providers to differentiate themselves through white labelling.
Furthermore, Enreach UP and Netaxis Fusion provide flexibility and customisation options for different market needs. Service providers can choose from a wide range of UC solutions that are tailored to specific segments, such as small businesses, enterprises, education, healthcare, hospitality, etc. Service providers can also integrate these solutions with other platforms or applications that their customers use. In this way, service providers can avoid investing in solutions that may become obsolete or incompatible over time.
Iain Sinnott, Head of International Carrier Sales, Enreach for Service Providers, said, “The combination of Enreach UP and Netaxis Fusion creates a powerful core for service providers who want to excel in the UC market. Think of this combined solution as a universal docking station, enabling technologies from multiple vendors to be easily accessible in one converged environment. Also, since our two companies carry out all the heavy lifting, we help service providers overcome barriers to adopting technology: the benefits have to outweigh the effort.”
In addition, the two organisations also believe that strong partnerships — with CSPs at the centre — are just as important as innovative technologies. “The industry needs to evolve beyond the basic model of a product vendor and service provider selling a solution to a customer. Instead, we need to widen the partnership model to include multiple technologies that address the changing needs of diverse customers and help CPSs differentiate while maintaining their independence and delivering positive customer outcomes. We want to create an ecosystem of partners, even including some with whom we compete: if we put the customer first, we can collectively succeed,” said Iain Sinnott.
Manuel Basilavecchia, CEO Netaxis Solutions, added: “We welcome this partnership and see a tremendous benefit for service providers by bringing the best together. We are in the business of helping to make the complex task of blending best-in-class solutions for CSPs simple. So, we are delighted to be working with Enreach, which clearly puts the CSP at the centre of the partnership model while also focusing on helping provide valuable customer outcomes. Fusion is part of our portfolio of applications and professional services, which we bring to this exciting next generation of technology integration and adoption.”
Note to editors
About Enreach for Service Providers
Enreach is a European leader in converged contact solutions. Our mission is to give companies access to the best communication and collaboration tools with a simple, user-centric interface built around their specific needs and systems. Our cloud UC platform Enreach UP enables service providers and integrators deliver their business customers value-added services, including FMC, video collaboration, messaging, inbound/outbound call centre functionality and conversational bots, seamlessly integrated with mobile services, Microsoft Teams, CRM and ERP systems. Enreach UP is offered as a multi-tenant, white label platform, with several deployment options for partners. Enreach group operates in over 25 countries and counts more than 1,300 employees. For more information visit: https://enreach.com/serviceproviders
About Netaxis Solutions
Netaxis Solutions, founded in 2010 by four telecom engineers, has over 50 employees, primarily engineers. Its head office is located in Brussels, Belgium, and it has branches in the Netherlands, Italy, France and the UK. Netaxis’ customers are Tier-1 telecom operators such as MTN, KPN, T-Mobile, Orange, Proximus and Vodafone. The company has strong partnerships with Enreach, Cisco and Oracle, whose products provide complementary services to customers in EMEA and Asia. Netaxis also serves large corporations and multinationals such as ABN Amro, ACHMEA, Vattenfall and Arcadis. More information at https://www.netaxis.be/
Dr. Sara McLin thought she made the right choice by going to an in-network emergency room near her Florida home after her 4-year-old burned his hand on a stove last Memorial Day weekend.
But McLin said a doctor there told her she couldn’t treat her son, Keeling, because he had second- and third-degree burns that needed a higher level of care. The doctor referred them to the burn center at HCA Florida Blake Hospital, about a 90-minute drive away.
McLin, who is a dentist, said the doctor told her the stand-alone ER would not charge for the visit because they did not provide treatment.
The stand-alone emergency room and ER doctor, who did not treat then-4-year-old Keeling’s burn last year and instead referred him to another hospital’s burn center, billed for his visit. But his mother, Sara McLin, initially could not dispute some of the charges — because her son’s name, not hers, was on one of the bills. (Zack Wittman for KHN)
Zack Wittman for KHN
“I don’t remember exactly how she phrased it. But something along the lines of, ‘Well, we won’t even call this a visit, because we can’t do anything,'” McLin said.
At Blake Hospital, she said, a doctor diagnosed Keeling with a second-degree burn, drained the blisters, bandaged his hand, and sent them home with instructions on how to care for the wound.
“I didn’t think anything more of it,” McLin said.
Then the bills came.
The Patient: Keeling McLin, now 5, is covered by UnitedHealthcare through his father’s employer.
Medical Service: From the stand-alone emergency room, none. A physician assessed Keeling and sent him to another facility for treatment. “Keeling needs a burn center,” the doctor wrote in the record of his visit.
Service Provider: Envision Physician Services, which employed the emergency room physician at HCA Florida Lutz Emergency in Lutz, Florida, near Tampa, and HCA Florida Trinity Hospital, the main, for-profit hospital to which the stand-alone emergency room belonged.
Total Bill: For the emergency room visit, Envision Physician Services billed $829 to insurance and about $72 to the family. HCA Florida Trinity Hospital billed Keeling about $129, noting it had applied an “uninsured discount.” An itemization showed the original charge had been nearly $1,509 before adjustments and discounts.
Keeling McLin, now 5, burned his hand on a stove last Memorial Day weekend. An emergency room doctor referred him to a burn center for treatment, and his family ended up getting billed for the ER visit, anyway. His mother initially could not dispute some of the charges because the bills were addressed not to her, but to Keeling. (Zack Wittman for KHN)
Zack Wittman for KHN
What Gives: The stand-alone emergency room and ER doctor, who saw Keeling but referred him to another hospital, billed for his visit. But McLin soon learned she was unable to dispute some of the charges — because her young child’s name was on one of the bills, not hers.
Months after the ER visit, McLin received a bill addressed to the “parents of Keeling McLin” from Envision Physician Services, the provider staffing service that employed the emergency room doctor who did not treat her son. She recalled the doctor’s promise that they would not be billed. “I should have made them write something down to that effect,” she said.
She said she called her insurer, UnitedHealthcare, and a representative told her not to pay the bill.
She received an insurance statement that identified the bill from Envision’s doctor — an out-of-network provider working in an in-network emergency room — as a “surprise bill” for which the provider may charge only copays or other cost-sharing under federal law. McLin said she had not heard anything since then about the bill.
After being contacted by KHN, Aliese Polk, an Envision spokesperson, said in an email that Envision would waive the debt, apologizing to Keeling’s family “for the misunderstanding.”
She described the ER doctor’s evaluation, determination, and referral as a medical service. She said the bill was for cost sharing for the visit — not the difference between what the doctor charged and what insurance paid, as the law prohibits.
“We recognize the patient’s family may have understood at the time of treatment that there would be no charge for the visit, including the medical service provided by our physician,” Polk said. “Unfortunately, this courtesy adjustment was not captured when the claim was processed.”
Maria Gordon Shydlo, a UnitedHealthcare spokesperson, said the insurer believed the matter had been resolved and did not follow up on requests for an interview, even after McLin waived federal health privacy protections, which would allow the insurer to speak to the reporter about the case.
McLin also received a bill from HCA Florida Trinity Hospital for its stand-alone ER at Lutz and decided to dispute the charges.
But after calling the hospital to appeal, McLin said, the billing department would not discuss the debt with her because the statement was in her young son’s name.
“They had him as the guarantor,” McLin said. Unlike Envision, which billed Keeling’s parents and their insurance, McLin said the hospital listed the child as “unemployed, uninsured.”
The child’s ER record also included his date of birth and doctor’s notes referencing his age. McLin said she wrote to HCA in November asking to appeal the bill and that a billing representative told her over the phone that it would put the debt on hold and review the dispute.
“I never heard anything back and assumed we were good,” McLin said.
Then, in January, she received a letter from Medicredit, a collection agency and an HCA subsidiary, stating that Keeling owed $129 and that he had until mid-February to contest the debt. KHN was unable to make contact with Medicredit representatives, and HCA Healthcare did not respond to requests for comment from its subsidiary.
Once again, Sara McLin’s name was not on the debt collector’s letter, and she said Medicredit representatives refused to discuss the debt with her because it was in her son’s name. She said she called HCA, too. “They said, ‘We can’t help you. We don’t have the case anymore,'” she said.
Erin Fuse Brown, a law professor and director of the Center for Law, Health & Society at Georgia State University, said McLin did everything right and that it is unusual for a parent to be barred from discussing a debt related to their minor child.
“The fact that the hospital wouldn’t even talk to her strikes me as the part that is absurd. It’s absurd as a business matter. It’s absurd as a privacy matter,” Fuse Brown said, adding that federal health privacy laws allow a parent or legal guardian to access their dependent’s medical information.
Fuse Brown said the hospital should have been able to correct the error quickly with more information, such as a birth certificate or other document establishing that McLin was Keeling’s parent. At the very least, she said, it could have given McLin notice before sending the bill to collections.
“You get the feeling that it’s this large, automated process, that there’s no human to get through to, that there’s no human to talk to and override the mistake,” Fuse Brown said. “Maybe it’s routine, but she couldn’t even talk to someone to correct a correctable billing error, and then the system just steamrolls over the patient.”
The Resolution: When the collection agency’s deadline passed without resolution, McLin said she felt frustrated. “Nobody can explain to me who has to approve talking to me,” she said. “I don’t know who that person is or what the process is.”
After KHN contacted the health system, HCA Healthcare canceled the family’s debt. HCA representatives declined to be interviewed on the record despite also receiving a privacy waiver from McLin.
“We have attempted to contact Mrs. McLin to apologize to her for the inconvenience this has caused her and to let her know that there is a zero balance on the account,” Debra McKell, marketing director for HCA West Florida Division, said in an email on March 3. “We also will be sharing with her that we are reviewing our processes to ensure this does not happen again.”
McLin later received a letter from HCA stating that the account had been cleared. She also said she received a call from a customer service representative informing her that the debt had not been reported to any credit agencies.
She said she was pleased, but that patients should not have to struggle to correct a billing error before it is sent to a collection agency and potentially ruins their credit.
“It’s the principle of the thing that’s annoying me at this point,” she said.
A billing mistake by an in-network Florida emergency room landed Sara McLin’s then-4-year-old son in collections.
Zack Wittman for KHN
The Takeaway: Though the notion of a debt collector pursuing a 4-year-old boy may seem farcical, it happens. When seeking medical care for a minor, it is important for the parent or guardian to ensure their name is listed as the responsible party.
Consumers who find themselves fighting a medical billing error need to “think like a lawyer,” Fuse Brown said, including documenting every interaction with the debt collector, getting any promises in writing, and recording phone calls. (State laws vary about how many parties on a call must give permission to record a conversation.)
Patients do not have to give up once a bill goes to collections, Fuse Brown said. “Once you hear from a debt collector, it’s not like the game is over and you lose,” she said. “Consumers do have rights.”
François de Brantes, a home health company executive and expert on how money flows through the health care system, said that hospital billing errors are not uncommon but that he had never heard of a situation like the one McLin experienced. He called it “puzzling” that HCA would issue a formal claim in a dependent child’s name.
De Brantes said those in a similar situation should also ensure that the collection agency removes any record of a debt against a minor to protect the child’s financial future.
“This stuff happens, where you have children who are improperly billed for stuff that they shouldn’t be billed, and they end up in collection,” he said. “Then the kid finds themselves with a collection record and they can’t get loans in the future, potentially student loans.”
Bill of the Month is a crowdsourced investigation byKHNandNPRthat dissects and explains medical bills. Do you have an interesting medical bill you want to share with us?Tell us about it!
KHN(Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs atKFF(Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Rural healthcare provider Mountainview Medical Center plans to break ground on a new $42 million replacement hospital in White Sulphur Springs, Mont., according to the website helenair.com.
Situated on 9.8 acres, the 45,000-square-feet hospital have 25 inpatient beds and offer acute care and nursing home care services.
The project received a $38 million loan from the U.S. Department of Agriculture Rural Development.
UnitedHealth Group and Cigna are revamping their prior authorization processes as new federal regulations aiming to ease the burden on providers and patients loom.
UnitedHealthcare will eliminate nearly 20% of existing prior authorizations beginning in the third quarter for its commercial, Medicare Advantage and Medicaid members, the insurer announced Wednesday. Next year, UnitedHealth will implement a national “gold card” program through which qualifying providers will simply notify the insurer about pending care rather than request prior authorization. This will eliminate the need for prior authorization in most case, according to the company.
UnitedHealth did not immediately respond to interview requests about why exchange plans were absent from these proposals, what procedures will be included, how it will determine eligibility for providers and how the notification process will work.
“We will continue to evaluate prior authorization codes and look for opportunities to limit or remove them while improving our systems and infrastructure. We hope other health plans make similar changes,” UnitedHealthcare Chief Medical Officer Dr. Anne Docimo said in a news release.
Cigna has removed prior authorization reviews for nearly 500 services and devices since 2020, Dr. Scott Josephs, national medical officer, wrote in an email. Approximately 6% of medical services are subject to Cigna’s prior authorization and the insurer uses an electronic process to enable fast responses to many requests, a spokesperson wrote in an email.
The health insurance lobbying group AHIP, Aetna, Centene, Elevance Health, Humana and Molina Healthcare did not immediately respond to interview requests.
Providers complain that prior authorization requirements have exploded in recent years, and that care is being delayed. For example, the Health and Humans Services Department’s inspector general reported last year that Medicare Advantage insurers improperly denied 13% of prior authorization requests.
The Centers for Medicare and Medicaid Services is slated to finalize proposals next month that would require health insurers to automate prior authorizations, process them more quickly, justify denials and publicly report data on their decisions.
This is a developing story. Please check back for updates.
Munich – China and Germany have further deepened cooperation at a regional level with a Tiexi Day event being held in Munich Germany on March 27, 2023.
The event coincided with an economic forum on Cooperation in the name of the China-Germany (Shenyang) Equipment Manufacturing Industrial Park.
Tiexi Day witnesses Sino-German Cooperation
With the theme of “China and Germany meeting, Seeing the Future”, the event attracted more than 100 representatives from the public and business sectors of both sides to talk about industrial cooperation and seek future development opportunities between China and Germany.
The event has witnessed signing of 11 projects, including the digital transformation and upgrading project of China-Europe Digital Alliance, the culture and tourism project of Kaiyuan Zhouyou Group Germany, and the strategic cooperation project between Kemether Automotive Engineering Technology (Liaoning) Co.,Ltd and Automation W+R GmbH.
Speaking at the event, Lv Zhicheng, Mayor of Shenyang introduced the city’s convenient investment environment and superior industrial park policies, welcoming German enterprises to invest in Shenyang. He also promised to “serve and support every enterprise”.
Chinese side also introduced the China-Germany (Shenyang) Equipment Manufacturing Industrial Park at the event. The park focuses on the development of intelligent and high-end equipment, automotive manufacturing, industrial services, strategic emerging industries, and currently has more than 470 enterprises, including more than 80 German companies. In the year of 2022, the park completed above-scale industrial output value of 86.4-billion-yuan, fixed asset investment of 19.5 billion yuan.
Germany is China’s largest economic and trade partner in the EU. The latest data from the German Federal Statistical Office shows that the bilateral trade volume between Germany and China reached EUR 297.9 billion in 2022, making China the most important trade partner of Germany for the seventh consecutive year.
There is a lot of hype around AI in healthcare and a rush of digital health companies seeking to cash in.
But experts are unsure how generative AI applications like ChatGPT and GPT-4 will influence clinical diagnosis and decision making. Most say the first wave of adoption will take place in areas where there are administrative redundancies.
Related: Microsoft, Nuance introduce ChatGPT successor to healthcare
“Obviously, there’s a lot of energy and a lot of concern,” said Dr. Greg Ator, chief medical informatics officer at University of Kansas Health System. “People just get way out in front of their skis on some of these technologies.”
Instead, early adoption of generative AI in healthcare is taking place in the less flashy area of clinical note taking. Ator is part of the team implementing generative AI technology at the academic health system to aid clinician note taking. The system is working with Abridge, a medical AI company, to summarize clinical conversations from recorded audio during patient visits.
Abridge’s generative AI technology is similar to Nuance Communications, a clinical documentation software company owned by Microsoft. Last Monday, Nuance said it is adding OpenAI’s ChaptGPT successor GPT-4 to its latest application, which will be used in electronic health record systems.
In both cases, users must describe what they’re seeing for the software to work properly. For example, if a patient presents with a sore throat, specific commentary of what the clinician is seeing must be verbally shared for the program to enter the information.
In addition to inputting relevant information to the EHR, both applications remove conversations not applicable to the care plan.
“They’re power tools,” said Abridge’s co-founder and CEO Shiv Rao. “[Generative AI is] a powerful tool in the context of a much bigger set of technologies that, orchestrated together, amounts to a solution that can create value in the workflow.”
Medical records are a logical place to begin because clinicians can quickly identify where AI-produced results were derived, Ator said. Clinicians can easily listen to a visit recording again if the AI misses valuable information.
“What you build beside, underneath and above these foundation models like GPT-4 is the secret sauce,” Rao said. “There’s a certain layer of technologies that are now available to all of us, but how we integrate those tools into larger solutions is going to be the difference between really magical experiences for doctors and their patients and solutions that feel like off-the-shelf toys.”
Investor interest remains strong
Investments in healthcare AI totaled $4.4 billion in 2022, according to data from Rock Health, a research and digital health venture firm. While last year’s total was down more than 50% from 2021, it was in line with 2020.
The same data revealed 2021 set a high watermark with 224 deals for companies using AI technology. While 2022 was not as fruitful, it was higher than 2020. Though experts say the levels from 2021 won’t be returning any time soon, the space remains of interest.
While AI investments have remained strong, few of those investments are ready for widespread adoption, skeptics say.
“I think that for some time forward, we’re going to continue to need to have humans in the loop because the AI is far from perfect,” said Erik Brynjolfsson, director of the digital economy lab at Stanford University’s Institute for Human Centered AI. “It can’t do a lot of things.”
Brynjolfsson said trained medical professionals are able to quickly dismiss abnormalities on a scan or medical image whereasAI may make a wrong diagnosis. While there is potential to eventually replace some roles of clinicians, experts say human input remains critical.
Generative AI is also time consuming to install and even in promising areas isn’t quite ready for primetime. Nuance is rolling out its GPT-4 feature in the summer.
Ator said University of Kansas Health System is implementing the technology over the few months. He is optimistic it will be completed by the end of the year, but did not want to provide a specific timeline. This is largely due to the time it takes to train clinicians and the integration required with the provider’s EHR platform Epic.
“Anytime you’re working with a complex system like, like Epic, which is our base medical system, we have to interact with them. Some of [the implementation] is driven by their timetable,” Ator said.
Another potential barrier to adoption could be patient acceptance. A Pew Research Center survey conducted in December found 60% of adult US patients would feel uncomfortable if their healthcare provider relied on AI for their medical care. Less than a third felt the quality of their care would increase as AI was implemented.
While the study did not specifically ask respondents about analyzing audio recordings of their visits, the report’s authors found “concern over the pace of AI adoption” was broadly shared in medicine.
Brynjolfsson said dictation and medical imaging are areas where providers could improve processes. But he said the future of healthcare will continue to require clinician and human oversight.
Others though are more bullish about future adoption.
“What we’re seeing today is just a sign of what’s going to come,” said Dr. Robert Pearl, the former CEO of Oakland, CA-based Kaiser Permanente and a current professor at Stanford University. “Everyone’s focusing on the mistakes of the day or the shortcomings of today. They’re irrelevant.”
Westcon-Comstor expands its AWS capabilities and commitment to help partners & their customers elevate security in the cloud.
SYDNEY, Australia – 28th March 2023– Westcon-Comstor, a global technology provider and specialist distributor, is proud to announce that it has earned Amazon Web Services (AWS) Security Competency status. This designation demonstrates Westcon-Comstor’s deep technical expertise and success in seamlessly delivering secure cloud solutions to its partners and their customers on AWS.
Achieving the AWS Security Competency differentiates Westcon-Comstor as an AWS Partner Network (APN) member that provides specialized software designed to help enterprises adopt, develop and deploy complex security projects on AWS. Westcon-Comstor has successfully met rigorous standards for security, compliance, and architecture, and has a proven track record of delivering secure and scalable cloud solutions to its customers.
“We are honoured to achieve AWS Security Competency status, a first for any distributor in APAC ” said Patrick Aronson, EVP, APAC and Global CMO Westcon-Comstor. “This recognition underscores our commitment to delivering secure, compliant, and innovative cloud solutions to our customers. With AWS, our customers can be confident in the security of their data and applications, and trust that Westcon-Comstor has the expertise to support their unique security needs.”
“Achieving the AWS Security Competency in the Identity and Access Management Category demonstrates Westcon-Comstor have deep technical expertise with AWS security and proven customer success securing the cloud journey with their vendor solutions and services offerings. We look forward to further accelerating AWS Partner success with Westcon-Comstor across the APAC region.” Jeremiah Jenson, Global Leader – Distribution at AWS.
“Westcon-Comstor provided us with the necessary support, expertise, and resources to successfully implement a DR solution and act as the communication channel between us and AWS.
Their team of technical experts were always available to answer our questions and provide assistance whenever we needed it. Our client is now benefiting from a highly resilient and scalable DR solution that meets their unique needs. The solution has helped us achieve our goal of ensuring maximum uptime for our client’s critical applications, which has increased their productivity and improved their overall customer satisfaction. Westcon-Comstor’s professionalism, and dedication to customer service were instrumental in our success, and we look forward to working with them again in the future.” Max Cheng, Senior System Engineer, Extranet Systems.
“Being awarded the AWS Security Competency highlights our local security expertise at partner’s disposal to help them analyse and secure their AWS infrastructure with our modern, leading-edge vendors. Through AWS, we can also access the latest security best practices and technologies, helping us to provide our customers with some of the most secure and scalable cloud solutions available.” Phil Cameron, Managing Director, Australia, Westcon-Comstor.
AWS is enabling scalable, flexible, and cost-effective solutions from startups to global enterprises. To support the seamless integration and deployment of these solutions, AWS established the AWS Competency Program to help customers identify Consulting and Technology APN Partners with deep industry experience and expertise.
About Westcon-Comstor
Westcon-Comstor is a global technology provider and specialist distributor, operating in more than 70 countries. It delivers business value and opportunity by connecting the world’s leading IT vendors with a channel of technology resellers, systems integrators and service providers. It combines industry insight, technical know-how and more than 30 years of distribution experience to deliver value and accelerate vendor and partner business success. It goes to market through two lines of business: Westcon and Comstor.
Piedmont Healthcare (Atlanta) is planning to transform the former Doctors Hospital on the Piedmont Columbus Regional Midtown in Columbus, Ga. The structure will become a freestanding children’s hospital named the Bill and Olivia Amos Children’s Hospital.
The 30-bed project will house a pediatric inpatient unit with several semiprivate sibling rooms. Additionally, the project includes isolation and behavioral safe rooms, a pediatric intensive care unit, and a pediatric intermediate care unit.
Support spaces include an activity room, laundry facilities, food pantry, room service dining, separate discharge area, and an outdoor playground.
A connection corridor linking to the Piedmont Columbus Regional Midtown main hospital is also planned.
The five-floor facility, slated to open in fall 2024, will be funded by a donation from the Bettye and Cecil Cheves family.
A novel bill making its way through the Tennessee General Assembly could have reverberating effects on Medicaid managed care procurement throughout the U.S.
Tennessee Speaker of the House of Representatives Cameron Sexton (R) and Speaker of the Senate Randy McNally (R), who also is lieutenant governor, sponsored the Tennessee MCO Reform Act, which would prohibit the state Medicaid agency from contracting with insurers that cover gender-affirming treatment for anyone, anywhere in the country.
Bills targeting transgender people have snowballed across Republican-led states. What started as restrictions on where transgender people can use the bathroom and what athletic teams they can join has escalated to legal restrictions on their medical treatment.
The Tennessee Legislature and Gov. Bill Lee (R) began the year by passing the nation’s first ban on drag performances in the presence of minors. More than 400 anti-LGBTQ bills are advancing through state legislatures this year, and 25 states have or are considering banning gender-affirming care for minors, according to the American Civil Liberties Union.
“We’re not particularly trying to fix a problem,” Tennessee state Rep. Tim Rudd (R), a cosponsor of the bill involving the Medicaid agency, said during a legislative hearing last month. “The way [gender-affirming care] is starting to be implemented is not within the values of most Tennesseans.”
The Medicaid proposal is a first-of-its-kind attempt to politicize the typically nonpartisan Medicaid bidding process, said Heather Howard, director of state health and value strategies at the Princeton School of Public and International Affairs. The legislation has massive market and legal implications and could revert TennCare, the first Medicaid managed care program, back to a fee-for-service model, she said.
The measure presents a litany of legal questions, many of which are already being considered in lower courts. For example, the bill invites challenges under the equal protection and interstate commerce clauses of the U.S. Constitution, the nondiscrimination provisions from the Affordable Care Act and Tennessee’s contractual obligations to the health insurance companies that provide TennCare benefits, policy experts said.
According to a nonpartisan Tennessee Legislature budget analysis, the bill would also limit the Medicaid agency’s ability to attract insurers to administer the program, which could simultaneously reduce quality and raise costs. In addition, any amendment to managed care contracts requires approval from the federal Centers for Medicare and Medicaid Services. If the terms are not approved and the state has no Medicaid managed care contractors, TennCare would have to shift to a fee-for-service model, according to the analysis.
“This would threaten to upend the entire notion of managed care, which relies on commercial insurers to come in. The theory has been—and Tennessee pioneered this—that these commercial insurance companies can provide greater value and slow the growth of costs,” said Howard, who previously served as New Jersey’s commissioner of health and senior services under Gov. Jon Corzine (D).
The Tennessee bill’s sponsors did not respond to requests for comment. Lee has not taken a position. “This bill is still moving through the legislative process, and as always, the governor will review final legislation when it reaches his desk,” a spokesperson wrote in an email.
A previous version of the Tennessee bill would have forbidden the Medicaid agency from contracting with insurers that offer surgery, hormone therapy and other gender-affirming treatments to anyone, including adults, through private and government-sponsored health plans. After revisions, the measure has a narrower scope and only seeks to exclude insurers that cover gender-affirming surgery.
Tennessee’s Medicaid program already bans coverage of gender-affirming care. This legislation seeks to influence insurers to extend that mandate to other product lines and states, said Lindsey Dawson, associate director of HIV policy and director of LGBTQ health policy at the Kaiser Family Foundation.
“This actually isn’t going to really impact access to care in TennCare because the services that we’re talking about are already not covered in the state, but it could impact contracts and services in other states,” she said.
If enacted, TennCare would have to revise its contracts within 30 days of the effective date to ensure compliance. Insurers would need to update care delivery protocols, claims processing systems and provider contracts to eliminate gender-affirming services or risk significant penalties, including lost contracts, Avalere Health consultant Michael Lutz wrote in an email.
If an insurer were deemed in violation, it would have 90 days to comply. Tennessee procured its multibillion-dollar managed care contracts last year, and terminating them to meet these requirements could affect continuity of care for all TennCare enrollees, Dawson said.
The money at stake for insurers may induce them to stop paying for gender-affirming surgeries instead, according to Lutz. “While the plans may disagree with the intent and impacts of the rule, the size of the revenue opportunity to serve the state would likely mean that the state would still be attractive to carriers,” he wrote.
Wellvana Health, a physician enablement company, has closed an $84 million capital raise, it said Monday. The round brings Wellvana’s total funding to approximately $140 million.
Kyle Wailes, CEO of the Nashville, Tennessee-based startup, said the funds will be used for growth and innovation. The capital raise was led by private equity firm Heritage Group and venture capital firm Valtruis. Houston-based nonprofit Memorial Hermann Health System also participated in the funding round.
Not a Modern Healthcare subscriber? Sign up today.
Wellvana provides data analytics, customer relationship management and population health technology to physicians and practices who are switching from fee-for-service to risk-based contracting models. It also offers practices boots-on-the-ground nursing care management services, coding assistance and more.
Most of the physicians it serves are independent, but some are employed by Wellvana itself or have come through partnerships with home-health agencies, skilled nursing facilities and health systems. The company operates in 22 states and will look for potential acquisition targets with these funds, Wailes said.
Since early 2022, digital health startups have dealt with macroeconomic headwinds and fewer opportunities to fundraise. The fourth quarter of last year saw the lowest quarterly digital health funding total since 2019. The failure of Silicon Valley Bank, which provided banking services to the digital health ecosystem, could lead to an even more challenging environment, experts say.
Wailes isn’t concerned about outside economic concerns and said the company had a strong financial runway.
“Our business model does extremely well in times of macroeconomic slowdown and inflation,” Wailes said. “It’s sort of a business model that’s recession-proof in many ways, but also inflation-proof as well because of how value-based care works overall.”
Axios reported in November that Wellvana was seeking strategic financing alternatives. Wailes did not comment on the specific report, but he said the company started the process of raising funds for this round in December.
Wellvana’s services cover around 100,000 Medicare and commercial lives through its various partnerships. It has three contracts with Medicare Accountable Care Organizations participating in the Realizing Equity, Access, and Community Health model. Wailes said half of the patients have come through the ACO Reach model.
“It’s a good program,” said Wailes, who was the former chief financial officer of the teledentistry company SmileDirectClub before taking over at Wellvana in January 2022. “It allows us to put more of a focus on patients with social determinants of health and how to better meet their clinical needs.”
Wellvana was founded in 2018 by Nashville-based Martin Ventures. Martin Ventures led former funding rounds with partnership from First Trust Capital Partners and Adam Boehler, who served as the first CEO of the U.S. International Development Finance Corporation under President Donald Trump.
That is the finding from a study by Jia et al. (2023) published last week. The authors find that:
Among 4003 eligible RCTs [randomized controlled trials], 1241 studies (31.0%) cited Cochrane reviews, 1698 studies (42.4%) cited prior non-Cochrane reviews, and 2265 studies (56.6%) cited either type of systematic review or both; 1738 RCTs (43.4%) cited no systematic reviews…the percentage of RCTs citing systematic reviews increased from 35.5% in 2007 to 2008 to 71.8% since 2020, with an annual rate of increase of 3.0%. RCTs with 100 participants or more, nonindustry funders, and authors from high-income countries were more likely to cite systematic reviews than those with fewer than 100 participants, industry funders, and authors from low- and middle-income countries.
This is a positive trend and one likely enabled by technology. As Google Scholar and PubMed databases have improved, as article search has become faster, both the cost (in terms of person hours) of conducting systematic literature reviews has likely gone down while the ease with which one is able to identify published systematic literature reviews has increased.
United States Catholic bishops have issued guidelines that seek to stop Catholic hospitals from providing gender transition care, a move LGBTQ advocates say could harm the physical and emotional health of transgender people within the church.
The 14-page doctrinal note, titled “Moral Limits to the Technological Manipulation of the Human Body,” sets forth guidelines for changing a person’s sex, specifically with youth. The document, issued Monday, says Catholic hospitals “must not perform interventions, whether surgical or chemical, that aim to transform the sexual characteristics of a human body into those of the opposite sex, or take part in the development of such procedures.”
Related: Catholic health organizations can deny trans care, court rules
Transgender Catholics have received a mixed response across the U.S. church. Some have found acceptance in specific parishes and rejection in certain dioceses, including those that bar church personnel from using trans people’s preferred gender pronouns. The bishops’ latest guidance to Catholic medical centers could prevent trans people from getting the health care they need, said Francis DeBernardo, executive director of New Ways Ministry, which advocates for greater LGBTQ acceptance in the church.
Catholic hospitals make up a sizeable portion of the U.S. healthcare system, and in some communities, they are the only option. The Catholic Health Association, which comprises more than 600 hospitals and 1,400 long-term care and other health facilities in the United States, says more than one in seven U.S. hospital patients is cared for in a Catholic facility.
“These decisions are being made at a much higher level without knowing the individuals and individual cases involved,” DeBernardo said. “When transgender people are not permitted or restricted from transitioning in ways they feel are appropriate, it could end in depression, anxiety or even self-harm, including suicide.”
The bishops’ guidelines “will not change much” when it comes to caring for transgender patients at Catholic hospitals, said the Rev. Charlie Bouchard, CHA’s senior director of theology and sponsorship. Transgender people will continue to always be accepted in Catholic hospitals and treated with dignity and respect, but might not receive all of the gender-affirming care they request because of the church’s theological and moral teachings, he said.
“As we look at the document from the bishops, what we are mindful of is that we have a history of caring for the marginalized, and we see transgender people very much as a marginalized group,” he said.
Not a Modern Healthcare subscriber? Sign up today.
Catholic hospitals see transgender patients with a variety of health care needs from broken bones to cancer treatment and heart attacks, Bouchard said, adding that the hospitals would not perform cosmetic procedures such as reconstructive surgeries, hysterectomies, or treatments such as sterilizations on request, unless there is a medical need for them.
He said Catholic hospitals are also training staff to be respectful of transgender patients: “When a patient checks in, we ask staff to be respectful in how they ask questions. We want to affirm transgender individuals as persons and provide them with spiritual care and psychological counseling.”
Bouchard said Catholic hospitals will “base health care on science and continue to follow the science when it comes to transgender people.”
“But we don’t treat ideology,” he said. “We treat patients who are really suffering. There are things out there about gender fluidity that we do not agree with. But as Catholic hospitals, we are held to the same standard of care as other hospitals.”
DeBernardo disagreed, saying the bishops’ doctrinal guidelines cause harm rather than heal people by not paying heed to science.
“The bishops’ unwillingness to counter any of the evidence from the scientific community or the experience of transgender people is neither good theology nor acceptable pastoral care,” he said.
Related: Minnesota governor signs executive order protecting gender-affirming care
DeBernardo said he sees hope with many more Catholics in the pews showing greater understanding of transgender people’s lives. He noted cases where Catholic parents are supporting their transgender children against restrictive policies in Catholic schools, including barring puberty blockers and preferred pronouns on campuses and in parishes.
Christine Zuba, a transgender woman who lives in New Jersey, said she feels accepted at her local parish, but is upset that the national church “continues to deny our existence and our need for health care.” Zuba said she was disappointed to see that transgender people were not even mentioned in the 14-page document.
“In my parish, I feel accepted unconditionally for who I am,” she said. “But that is missing in our hierarchy. There is no willingness to engage with us and understand our lives.”
Zuba said she is happy to see more engagement and interaction in some dioceses. In Davenport, Iowa, Bishop Thomas Zinkula formed a Gender Committee calling Catholics to “listen to the people in the margins,” calling ministering to LGBTQ people – particularly trans people – as “a life issue.” In a column published in the Catholic Messenger, Zinkula said he has been haunted by the story of a transgender youth who attempted suicide after being denied Communion.
“This type of thing should never happen again,” he wrote.
Zuba said she would like to see that type of commitment to listen and learn in the upper echelons of the church.
“All we ask is listen to us as a group and as individuals,” she said. “Open your hearts and try to understand.”
Download Modern Healthcare’s app to stay informed when industry news breaks.
Situated on the third floor, the project combined two medical and surgical units into one new department with 46 private inpatient rooms, a six-room post-surgical recovery area, two nurses’ stations, visitor lounges, and a family conference room.
The surgical specialty unit offers treatment for patients recovering from general, cardiovascular, cancer, bariatric, and gynecological surgeries.
Authorized generics (AGs) are generic drugs that–unlike independent generics–are sold by the brand-name drug manufacturer under a generic label. How big a role do these AGs play among Medicaid beneficiaries. A paper by Rome et al. (2023) aims to answer that using public Medicaid prescription use data between 2014 and 2020. Using these data, they find:
From 2014 to 2020, 1023 AGs accounted for 175 million filled Medicaid prescriptions. These represented 4% of Medicaid prescription drug use, and 16% of medication use among products with AGs available. Among 393 AGs for drugs without generic competition before 2014, 139 (35%) were marketed at least 1 year before independent generics or had no independent generic competition through December 2020…AGs represented a small share of Medicaid prescription drug use from 2014 to 2020, but when AGs were available, they accounted for sizeable market share.